Jeffrey - known for his work in promoting the Artificial Pancreas concept and project at JDRF during his time there - spoke eloquently about how T1D "eats away at quality of life" and how Bigfoot was committed to giving some of that "T1D" time back to PWD and their families.
In terms of technology, it was evident that the smartphone was going to be central to their system, with components connected through the Bluetooth Low Energy (BLE), also known as Bluetooth Smart, protocol. Insulin bolusing and management will be on the paired smartphone. So what happens if you lose / break the phone? As you'd expect, for such a safety-critical system, Jeffrey confirmed that insulin delivery will continue and the core pump will be smart enough to work without a phone (you can also pair another phone).
 |
| The Smartphone: at the centre of the Bigfoot tech system (an excuse to show the Fairphone 2) |
And all this tech will be surrounded by an intuitive user interface, designed to be simple and easy to use (Jeffrey made the point that you don't get a manual with an iPhone...) But he said that Bigfoot aren't [primarily] a medical device company. It was clear that Bigfoot intends to deliver more than just a device.
They intend to deliver a diabetes management service.
Genius.
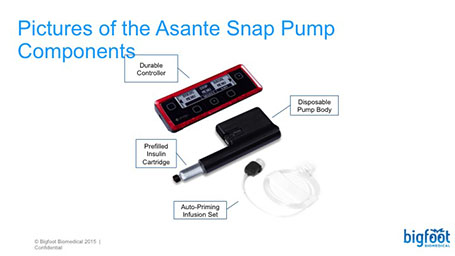
For one monthly fee - and Jeffrey suggested this would be less than the effective cost of a sensor enabled pump - Bigfoot would provide the kit (your pump, CGM transmitter, sensors, a BG meter, test strips, infusion sets) but also look after managing consumables for you. I guess if they provide everything, and all the data goes up to the cloud, they know how many sensors you've gone through, how many infusion sets (including knowing which ones have failed and texting you to warn you before you might otherwise notice the thing is kinked - our favourite way of failing) etc. They'll manage your T1D stock [not sure how this would work in the UK, with some supply costs coming from our primary care providers, others via the diabetes clinic and some from our own pockets, but it's got to be doable].
Medtronic, here in the UK, rightly patted themselves on the back for setting up an online store, but this is potentially miles better and one less thing to worry about. [Medtronic UK appear to thinking along these lines at least - see https://www.facebook.com/MedtronicDiabetesUKandIreland]
And, of course, Bigfoot can also leverage the skills and experience of the other key founders (Bryan Mazlish, Lane Desborough and Jon Brilliant). Bryan Mazlish is famous for running his own DIY closed-loop artificial pancreas setup within his own family (on both his wife and son). Jeffrey revealed that the Bigfoot team were not going to use clones of Brian's system themselves (despite the obvious benefits that would on its own), but would rather wait and deliver their complete system to everyone. That's a pretty amazing commitment. That's like typing away late at night, knowing there's a pack of Chocolate Hob Nob biscuits in the house, but not going to get one until a post is finished....... sorry, where was I?
Jeffrey made the point that closed loop systems have proven themselves in a variety of outpatient settings around the world. But despite this, the big players, the big pump companies, appear - at best - to be inching towards an AP solution.
He also made the great point that these AP systems will not just operate in isolation, but will be connected to the cloud, where big data can be leveraged to improve the health, quality and safety of T1D of PWD and their families.
So when should we expect to see the Bigfoot service?
Looking at the end of 2018 for FDA approval.
As you'd expect, there's a ton of testing to be done - expect to see inpatient, then outpatient trials, followed by the pivotal trial, the latter devoured by the FDA for evidence that it should approve Bigfoot's service.
Interesting, Jeffrey, was at pains to point out that the FDA were collaborating fully. He stated that the "FDA has made all this possible", in terms of making Bigfoot a viable concept, in regulatory terms. Responsibility for success was now clearly with the companies - and not the FDA: "the FDA are not standing in their way."
In response to a chat room question, he highlighted the different approaches taken by EU and US regulators and thought examples of "EU first" approval was purely due companies planning it that way. Incidently, with the exception of Dexcom he wasn't overly positive about how companies were engaging with the FDA (a view I've heard expressed elsewhere too).
This doesn't all come together overnight. Bigfoot have to keep their eye on lots of moving targets and this is obviously a hugely complex problem. Their solution has to demonstrate it's making T1D easier to manage for patients and clinicians - and it doesn't add any additional burden to the overall healthcare economy (ie eventually show APs like this will keep people out of hospital and reduce complications). That's a big ask. Jeffrey mentioned it might take ~$100m (compared to the $10m raised to date by Bigfoot).
I was really impressed by the combination of achievable technology gains and practical help in the form of the service described, rather than just a device with a helpline and a manual. Jeffrey conveyed a deep and personal understanding of T1D problems, as you might expect from his background in JDRF and as a parent of a son with T1D since 2002. But I also sensed this permeated through the company, from staff members with T1D and those caring for others with T1D (over half of the 34 strong workforce). In a relatively small company, that could turn out to be Bigfoot's biggest advantage.
As ever, feel free to post a comment below, on Facebook or on Twitter :-)
Let me know when you go public. My husband sold my dexcom stock against my will. He was foolish, IMHO, for my strong "go with what you know" foresight. Never again, I say!!
ReplyDeleteThe plan to secure reimbursement is the critical path for this tech. Hoping that these discussions have already commenced.
ReplyDeleteGood point Kevin: fingers crossed the discussion has indeed begun, in the US at least. Not only do all the individual pieces of tech have to bolt together to form a tech system, it has to force itself into the healthcare system itself. If it's a penny more expensive than what is replaces, it'll have to be able to demonstrate to commissioners (within the NHS at least) that it offers the best value for money.
DeleteWhilst we wait for the AP, we're doing our best to manually sugar surf Kevin :-) Thanks for all the tips and advice you guys have shared.